There is a well established evidence suggesting that surgery and anesthesia have a significantly impact on the patients’ neurocognitive recovery What is debatable is the connection between the long-term cognitive functioning and emergence of neurodegenerative disorders, such as Alzheimer’s or Parkinson’s disease several years after exposure to a para-surgical insult This is of particular interest in the field of pediatric and geriatric medicine. The potential detrimental effect on long-term cognitive performance may be more profound in younger subjects. Others researchers believe that younger individuals have a higher capacity to withstand the para-surgical stress unscathed. On the other part of the age spectrum, elderly subjects, or individuals with pre-existing cognitive impairment, may be uniquely vulnerable to the potential detrimental effect of anesthesia and surgery. The effect of para-surgical stress can interact with surgical comorbidities including malnutrition, deconditioning, inflammation, and sepsis (4, 10). The debate is far from being concluded, but the preservation of cognitive function is gaining increasing importance as reflected in several initiatives. Therefore, there is a great need to understand this clinical sequalae after surgical insult.
In this study, we investigated the dynamics of four markers of neurological injury after heart surgery involving cardiopulmonary bypass. tau protein is well-known markers associated with Alzheimer’s disease (AD).
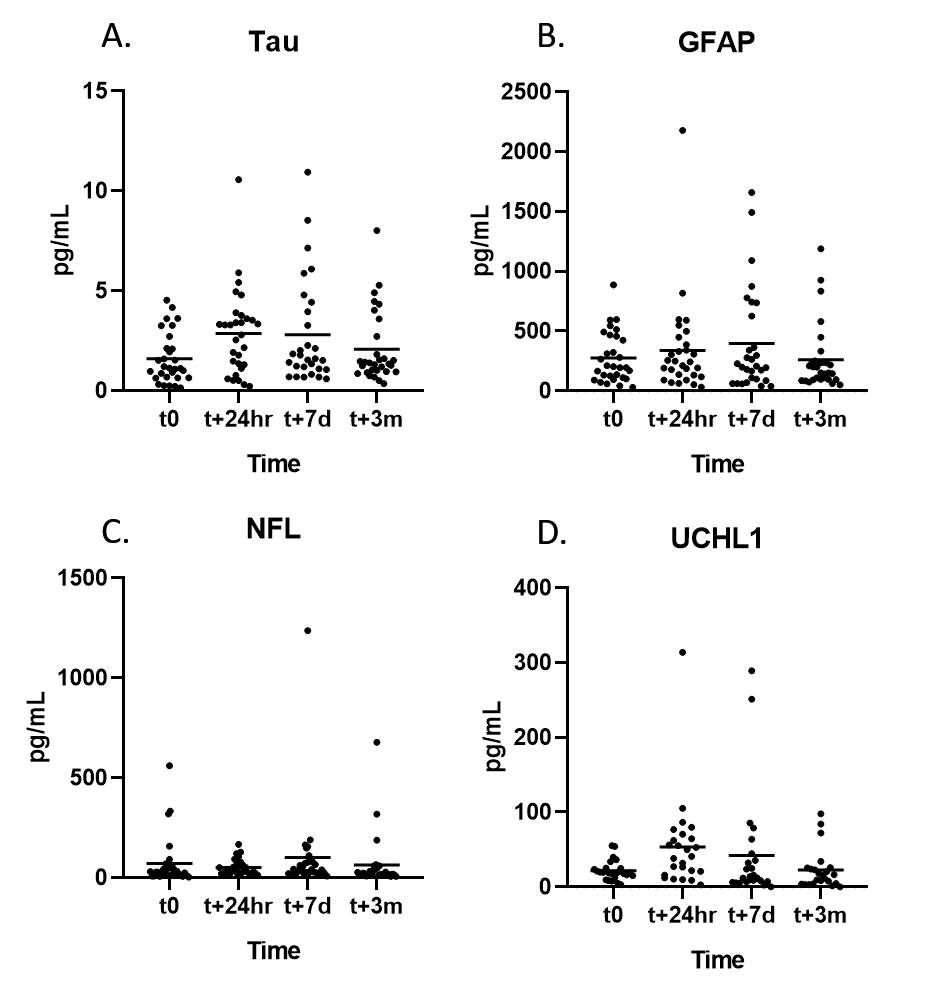
Serum NF-L peaked at 7 days (p = 0.044), while UCH-L1 peaked at 24 hours (p = 0.0011). Both of these levels normalized at three months. Serum level of tau protein increased 24 hours after surgery (p=0.008) and remained elevated at seven days (p = 0.0125) and three months (p = 0.023). In vitro secretion of M-CSF by lipopolysaccharide stimulated peripheral monocytes, but not TNFα, correlated highly (r = 0.58; p = 0.04) with persistent elevation of serum tau level at three months. Correlations of CRP and SAP but not α2M with serum tau post-CPB increase were statistically significant.
Our study aimed at
understanding the dynamics of neuroinflammatory markers among individuals
undergoing cardiac surgery with application of CPB. We yielded significant results which were
partly consistent with prior documented data while providing new findings Most
importantly, our study demonstrated a delay in the peak time of neurodegeneration
markers which could be a factor of CPB implementation. While the rise in
neuronal injury markers has been well documented in prior studies, its
elevation was not documented past the 72 hours post insult. This also calls for
further investigation which could potentially involve a longitudinal follow up
of individuals undergoing cardiac surgery with CPB.